
A small case series showed that the long-acting injectable regimen Cabenuva led to viral suppression in all 12 people whose HIV was not kept in check with daily oral antiretrovirals, according to a recent report in Clinical Infectious Diseases.
Despite remarkable advances in antiretroviral therapy (ART), easier and more accessible treatment options are still needed, as only about two thirds of people diagnosed with HIV in the United States have achieved viral suppression.
In 2021, the Food and Drug Administration (FDA) approved Cabenuva (injectable cabotegravir plus rilpivirine), which is administered by a health care provider once monthly or every other month, as the first complete antiretroviral regimen that does not require daily pills. To date, it is approved only as a switch option for people who already have an undetectable viral load and have no known or suspected resistance to cabotegravir or rilpivirine.
Two Phase III clinical trials showed that Cabenuva is highly effective for people who have already achieved viral suppression. The ATLAS study evaluated the regimen as maintenance therapy for treatment-experienced people who had a stable undetectable viral load on a standard oral regimen. The FLAIR study enrolled previously untreated people, but they achieved viral suppression on a short-term oral regimen before switching to the injections.
Emerging evidence suggests that Cabenuva may also be a viable option for people starting treatment for the first time and for those who have been unable to maintain viral suppression using existing oral regimens due to difficulties with adherence or other challenges.
Monica Gandhi, MD, MPH, and her team at San Francisco General Hospital’s Ward 86 clinic—which serves the city’s most disadvantage people with HIV—found that 12 of the 15 people who started Cabenuva with a detectable viral load in a pilot study achieved viral suppression, some of them for the first time.
At this year’s Conference on Retroviruses and Opportunistic Infections, Gandhi reported results from a larger group of 133 people. Most (88%) were cisgender men, the median age was 45 years, 38% were Latino, 32% were white and 16% were Black. Two thirds were unstably housed or homeless, a majority reported active substance use and more than a third had major mental illness. Almost all were covered by Medicaid, Medicare or both. A majority (76 people) already had an undetectable viral load on oral meds, and all of them maintained viral suppression after switching to the injections. The more exciting finding was that all but two of the 57 people who started Cabenuva with a detectable viral load—some of whom had advanced immune deficiency—achieved viral suppression.
During a discussion after the presentation, some audience members wondered whether this could work without the kind of intensive support available in San Francisco. Ward 86 offers services including case management, phone or text reminders of upcoming injection visits, follow-up for those who miss appointments and even street-based nursing services. The city offers excellent HIV care overall and provides extensive services for people experiencing homelessness. Unlike some other states, California covers Cabenuva through Medicaid and its AIDS Drug Assistance Program.
Now, a new analysis by James Brock, MD, and colleagues from the University of Mississippi offers evidence that the approach is also feasible in a different setting that also offers intensive support.
The Adult Special Care Clinic, a Ryan White-funded HIV clinic at the University of Mississippi Medical Center in Jackson, has been offering Cabenuva as a “salvage” option for people who have not achieved sustained viral suppression despite optimized oral antiretroviral therapy and intensive case management.
Between February 2022 and June 2023, 12 people with persistent viremia started Cabenuva. Seven were cisgender women, five were cisgender men and the median age was 42 years; 11 were Black and one was Native American. Here, too, most were covered by Medicaid or Medicare. Four had major mental illness, and three had a substance use disorder, but only one reported unstable housing. At baseline, 10 people had resistance-associated mutations, including four NNRTI and five integrase inhibitor mutations.
Six people initially started Cabenuva injections every month. All of them achieved viral suppression and then transitioned to injections every two months. Based on this favorable experience, the remaining six participants started with injections every other month after receiving loading doses for the first two months. Overall, virologic outcomes were “excellent,” the authors reported. All patients achieved an undetectable viral load (below 50) within three months of starting Cabenuva, and none experienced viral rebound.
Despite historical poor adherence to oral antiretrovirals, adherence to Cabenuva was described as “very good,” with just five out of 82 injection visits occurring after the scheduled window. None of the late injection visits resulted in viral rebound. No participants discontinued Cabenuva due to attrition, virologic failure or side effects.
What’s more, CD4 T-cell recovery was also good. At baseline, the mean CD4 count was only 233, and five participants had a current AIDS diagnosis. The mean CD4 gain was 184 cells, and people with a count below 200 experienced more than a 300% increase, on average. Three patients with evidence of wasting gained up to 15 pounds.
Implementation of this program has required close collaboration among clinicians, case managers and pharmacists, the report authors noted. Although Cabenuva is included on Mississippi’s Medicaid preferred drug list without viral suppression restrictions, obtaining approval through other payers has required peer-to-peer discussions after initial denials. Case management involves regular telephone follow-up, appointment reminders and transportation assistance. The Adult Special Care Clinic’s injectable ART program now has a full-time registered nurse for case management and injection administration. Nonetheless, barriers to care are common, including lack of transportation and inconsistent phone service.
In summary, these findings further support the use of long-acting injectables for people without viral suppression. “This regimen has been utilized in our practice as a salvage option for people with long-standing viremia and often advanced disease, where the potential benefits of virologic suppression far outweigh the risks of treatment emergent resistance,” the authors wrote. “Directly observed therapy through [every other month] injections provides a much-needed therapeutic option for thousands of people in the United States who have not achieved virologic suppression.”
Time to Change the Guidelines?
The FDA is reluctant to approve additional indications—and panels that develop treatment guidelines are hesitant to change practice—without data from controlled clinical trials. But people who have not been able to achieve and maintain viral suppression are in most dire need of new options, and randomized trials comparing oral versus injectable treatment may not be possible for those who are unwilling or unable to take daily pills.
Yet given the accumulating evidence from small studies such as these—as well as a modeling analysis suggesting that Cabenuva with wraparound services would improve viral suppression and life expectancy compared with oral integrase inhibitors—some experts are ready to take the plunge.
Use of long-acting CAB-RPV in PWH and virologic failure is specifically discouraged in HIV treatment guidelines.
— Paul Sax (@PaulSaxMD) September 22, 2023
But there are rare situations where this is the *only* option -- and it can be life-saving. Time for a guidelines change? I’d vote yes. https://t.co/WAur5Day2V
1/5
“If the alternative is untreated and progressive HIV disease, and the patient has advanced immunosuppression, we should stop discouraging use of this potentially lifesaving therapy,” Paul Sax, MD, of Brigham and Women’s Hospital, wrote in his New England Journal of Medicine Journal Watch blog, stressing that this is his opinion, not the position of guidelines panels he serves on.
“The experience with these dozen [Mississippi] patients is now being reproduced anecdotally in small case numbers from other centers, including our own,” he continued. “While San Francisco led the way, this is doable in any HIV treatment clinic with intensive case management services.”
Currently, the Department of Health and Human Services HIV treatment guidelines state that Cabenuva (CAB plus RPV) is not recommended for people with virologic failure. The IAS-USA guidelines take a similar position.
Sax offered a proposed revision to the guidelines:
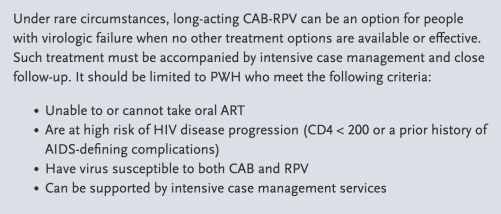
Courtesy of Paul Sax
“Sure, there will be cases where treatment failure with resistance occurs; where patients are lost to follow-up; where we will need to battle with payers to convince them to cover this non-FDA-approved indication; where the team of people (and it’s always a team) charged with case management and medication administration spend enormous time and energy to no avail,” he wrote. “I acknowledge these issues and frustrations, but at the same time, ask—what is the alternative? It can’t be to withhold the only regimen that might help them.”
Click here for more news about HIV treatment.




Comments
Comments